- 800.525.2690
- [email protected]
- Mon - Fri: 8:00 - 4:30


Note: This article describes the Minuendo product. Click here to learn more about Minuendo.
Reposted with permission from original author, Robert Traynor
Introduction
Tidball and Fagelson define decreased Sound Tolerance (DST) as an abnormal physical and emotional response to routinely experienced sounds.1 It is an auditory complaint arising from damaging sound exposure, physical disease or dysfunction, mental health conditions, injury, or as a side effect of some medications. Patients may find these sounds merely irritating, or they may have a more ominous reaction, experiencing severe discomfort or even pain upon exposure to certain signal combinations. Decreased sound tolerance often causes people to have an exaggerated startle response to sound that may lead to isolation, distress, anxiety, and the inability to concentrate, affecting performance at school or in the workplace. The normal reaction to decreased sound tolerance leads to the overuse of sound attenuation created by hearing protection devices.
Incidence
While the average audiology practice may see an adult patient with decreased sound tolerance infrequently, they are seen routinely in tinnitus clinics. In addition, among children, speech-language pathologists encounter decreased sound tolerance cases more than expected as part of their caseload in schools or other clinical situations.
The American Tinnitus Association (ATA) estimates that the prevalence of hyperacusis (another term for sound tolerance) range from 7.7–15% of the population.2 Twelve percent of ATA members report having hyperacusis symptoms. Recent data by Baguley offered insight into the incidence of decreased sound tolerance from a Swedish study where 9.2% of adults self-identified themselves as having decreased sound tolerance.3,4

Another investigation from the UK surveyed 7,000 11-year-old children, finding that 3.7% of the respondents described sound tolerance as an issue.5 Baguley emphasizes that since most elementary schools have a class size of about 30 students, this study would suggest that one student in every class would likely display some degree of sound tolerance problem.3
Among children with Autism Spectrum Disorder (ASD) the incidence of sound tolerance was found to be 18%.6 Recently, Williams, in a meta-analysis of interviews and observations of patients with ASD, found that 27.3% experienced decreased sound tolerance problems suggesting almost 10% higher than previous indications.7 Thus, current epidemiology available for decreased sound tolerance disorders suggests a significant occurrence in adults, normal children, and special needs children.
Self-Treatment with Attenuation is a Clinical Problem

Clinically, when adults or children present themselves for sound tolerance disorders, they are often self-treated with hearing protection devices (HPDs) and develop a dependence on these devices.8 These may either be passive traditional devices used in industry or the newer types of electronic headphones or earbuds. Littwin offers personal experience with sound attenuation submitting “that the use of hearing protection devices is seductive as they allow for less pain and discomfort around sound and offer a measure of control.”9 For children, Kennedy et al state that, “the use of ear defenders or earplugs to reduce the volume of sounds seems to be commonsense to those seeing a child distressed by loud sounds.10 Evidence shows that the ensuing auditory deprivation, although well-intentioned, can sensitize the auditory system.”11 Studying this issue, Formby et al. concluded, “the use of HPDs to control sound tolerance could be overused and may exacerbate sound tolerance issues.”12 Baguley and Andersson present that literature suggests, “hyperacusis is likely a disorder created by an abnormally high central auditory gain.13,14 Thus, it is logical that the changes were seen anecdotally and in research studies would indicate that reducing the intensity of the environmental sound further increases central auditory gain due to the auditory system attempting to compensate for the reduction of sound input.”
Since the increased central volume and, therefore, increased sound sensitivity is why HPDs are used, clinicians and researchers worldwide overwhelmingly agree with Baguley and Andersson that “patients should be counseled to wean themselves off the use of these devices.”13 Evidence indicates that sound tolerance difficulties are only exacerbated using attenuation devices. Thus, gradual movement from hearing protection devices is essential before initiating sound therapy, cognitive behavior, or other therapies for decreased sound tolerance.
A Possible Solution

Initially designed for the music industry to provide a variable, high-fidelity, flat response attenuation of a sound landscape for musicians, these new variable attenuation hearing protection devices may have a clinical application. These devices may not only temporarily offer relief to those with decreased sound tolerance, but their easy attenuation variability allows for the gradual movement toward normal sound sensitivity and, ultimately the cessation of use.
Figure 1 presents the response curve of new, variable attenuation musician plugs at three stepless settings with mean real measures when closed at approximately 25 dB, 14 dB at midpoint 14 dB and, 7 dB when open.
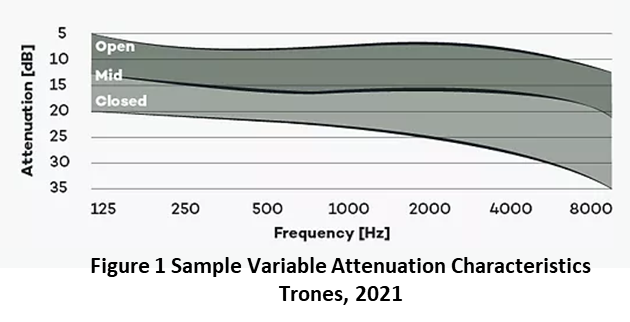
Trones indicates that true variable attenuation is obtained due to a variable membrane that allows a flat response across the frequency range like a “second eardrum” where the tension can be continuously controlled to create various degrees of attenuation (Trones T. Personal Communication, April 2021). Some “variable plugs” use older technology that incorporates ports and vents that vary the device’s seal, compromising sound quality. Using these innovative new HPDs offers the patient control over the amount of attenuation. Although gradually reducing HPD attenuation may be enough to facilitate effective sound tolerance treatment for some, others may require more sophisticated treatment such as Sound Therapy or possibly Cognitive Behavior Therapy.
Summary
In this new century, wearing technology is common. Fashion conscientious consumers now routinely wear earbuds, air pods, hearables, and other devices in their ears which have become a normal part of daily life. Adults, children, and those with special needs will readily adopt a high-tech-looking device rather than traditional plugs or earmuffs that make them either look strange or different. Unknown to the public, these patients will be weaning themselves from the constant deep attenuation that creates the cycle of more auditory sensitivity. While musicians may use these variable attenuating hearing protection devices, they offer a significant clinical application in treating those with sound tolerance disorders.
References
- Tidball G, and Fagelson M. Audiological Assessment of Decreased Sound Tolerance. In M. Fagelson and D. Baguley, (eds), Hyperacousis and Disorders of Sound Tolerance, San Diego: Plural Publishing; 2018.
- American Tinnitus Association. Understanding the Facts: Related Conditions, Hyperacousis. 2021. Retrieved April 27. Available at: https://www.ata.org/understanding-facts/related-conditions
- Baguley D. 20Q: Current perspective on Hyperacousis. In G. Mueller, Ed, 20Q, Audiology Online, October 2017.
- Paulin J, Andersson L, Nordin S. Characteristics of hyperacusis in the general. Population, Noise & Health 2016;18:178–84.
- Hall A, Humphriss R, Baguley D, Parker M, and Steer C. Prevalence and risk factors for reduced sound tolerance (hyperacusis) in children. Int J Audiol 2016;55(3):135–41.
- Rosenhall U, Nordin V, Sandstrom M, et al. Autism and hearing loss. J Autism Developmental Disord 1999;29:349–57.
- Williams Z and Suzman E, and Woynaroski T. (2021). Prevalence of Decreased Sound Tolerance (Hyperacusis) in Individuals with Autism Spectrum Disorder: A Meta-Analysis. Ear and Hearing 2021;42(1).Retrieved April 9, 2021,
- Searchfield G and Selvaratnam, C. Hearing Aids for Decreased Sound Tolerance and Minimal Hearing Loss: Gain without Pain. In M. Fagelson and D. Baguley, (eds). Hyperacusis and disorders of sound intolerance: Clinical and research perspectives. Plural Publishing; 2018.
- Littwin R. Hyperacusis Management. In M. Fagelson and D. Baguley, (eds). Hyperacousis and Disorders of Sound Tolerance, San Diego: Plural Publishing; 2018.
- Kennedy V, Benton C, and Kentish R. Increased Sound Sensitivity in Children. In M. Fagelson and D. Baguley, (eds), Hyperacousis and Disorders of Sound Tolerance, San Diego: Plural Publishing; 2018.
- Munro K and Blout J. Adaptive plasticity in brainstem of adult listeners. J Acoust Soc Am 2009;126(2):568–71.
- Formby C, Sherlock, L, and Gold S. Adaptive plasticity of loudness induced by chronic attenuation and enhancement of the acoustic background. Acoust Soc Am; 2003;114:55–58.
- Baguley D and Andersson G. Hyperacousis: Mechanisms, Diagnosis, and therapies. San Diego: Plural Publishing; 2007.
- Pollard, B. (2021). Definitions. Focus on Hyperacousis, Retrieved April 15, 2021 from: https://hyperacusisfocus.org/research/definitions/
Originally published in Canadian Audiologist.